Ileal Pouches: An Overview
Some cases of colorectal diseases make it crucial for the patients to undergo the total proctocolectomy, which is a surgical procedure aimed at removing the entire colon and rectum. This surgical removal of the large intestine may make a patient eligible to undergo another surgical procedure known as ileal pouch-anal anastomosis (IPAA). The IPAA refers to the construction of an internal reservoir that empties into the anal canal, allowing the patient to get rid of bodily wastes through the anus.
What is an ileal pouch?
Your doctor may recommend a total proctocolectomy if you are a patient of ulcerative colitis, familial adenomatous polyposis, or colorectal cancer. This surgical procedure will involve the removal of the entire colon and rectum.
Following this procedure, the patient may qualify for another surgery known as ileal pouch-anal anastomosis (IPAA), which connects the small intestine to the anal canal to allow the patient to expel bodily wastes through the anus.
The terms ‘anastomosis’ refers to the construction of a reservoir by folding the end of the small intestine and suturing the combined sides of the fold. This reservoir fits over the anal canal, meaning that you will feel the need to move your bowels when the pouch is full. This way, you will not need to wear an external bag to manage your stool evacuations.
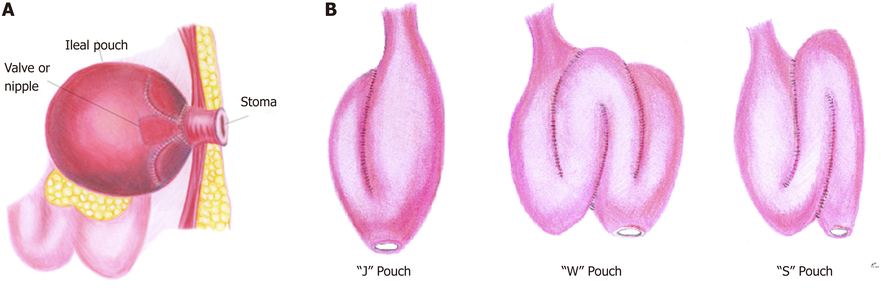
The three types of ileoanal pouch include a J-pouch, S-pouch, and W-pouch. The J-pouch is more common as it needs the shortest length of the small intestine during the construction of the reservoir.
The most essential prerequisite for the creation of an ileal pouch is the good health of the small bowel, sphincter muscles, and pelvic nerves. It will allow the patient to have control over when to move bowels.
Different types of ileal pouches
The first type of ileal pouch to talk about is the j-pouch, which consists of two loops of the small intestine combined to form a reservoir. The surgeon fits this reservoir over the anal canal to allow the patient to get rid of bodily wastes through the anus. The reservoir holds the stool until it becomes full, after which the patient feels the urge to go to the toilet. People who have a j-pouch may have to visit the bathroom 6-8 times a day. The number of days reduces when the internal reservoir expands, and the consistency of stool thickens.

An S-pouch works the same way as that of a j-pouch. The only difference is that it has an ‘out-spout’ below to pouch to compensate for the shortage of the length of the small intestine. The problem with an S-pouch is that it might make it difficult for the patient to get rid of bodily wastes completely. It may necessitate the insertion of tubing into the pouch through the anal canal to draw wastes out.
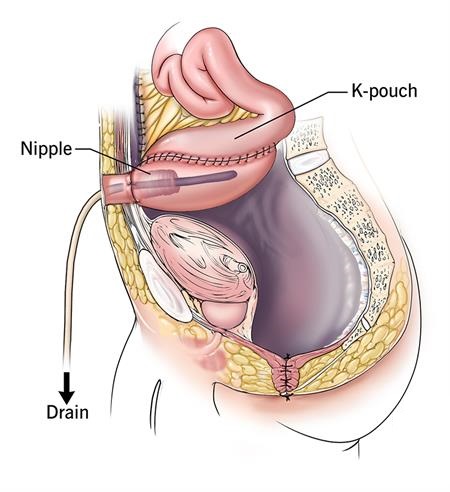
Another quite common kind of ileal pouch is the Kock pouch or K-pouch. This option is for the patient whose anal sphincters and other related organs are not fit enough to allow a comfortable removal of bodily wastes through the anus. A Kock pouch may be helpful in this regard because it also eliminates the need to wear an ostomy pouch over the abdominal opening. This internal reservoir connects to the abdominal opening through a valve consisting of living tissues from the ileum. This self-sealing valve does not allow waste materials to leak from the opening, giving the patient complete control over when to get rid of bodily wastes. All you have to do is to insert a catheter into the internal pouch through the opening and draw wastes out of the body.
Which option right for you depends on your health and other factors that your doctor will look at while analyzing your case.